
Running Injury Series | Blog 1 of 6 | All levels | 15 min read
By Simone Passeri — HCPC Physiotherapist & MSc Sports Therapist | May 2026
Why runners get injured.
Running is one of the most accessible sports in the world. You don’t need any special kit, a gym membership, or even a coach! So, perhaps it’s not surprising that running-related injuries are common; studies have estimated that around 40% of recreational runners sustain a running-related injury each year (Kakouris et al, 2021). So how can you stay fit, healthy and injury free?
For details of how we can work with you, visit our Physiotherapy main page https://www.evolverehabtherapy.co.uk/physiotherapy-and-sports-therapy-2/
This is the first blog in a six-part series on the fundamentals that underpin nearly all running-related injuries. Whether you are dealing with knee pain, Achilles issues, shin splints or plantar fasciitis, the root cause often comes back to the same principles. Understand these and you will not only recover faster when things go wrong — you will also run further, faster and more efficiently when things go right.
Contents:
- Overuse Injuries: How Running Injuries Really Develop
- The Single Biggest Risk Factor: A Previous Injury
- The Two Loads Every Runner Needs To Understand
- The Acute:Chronic Ratio
- Why The Same Training Error Causes Different Injuries
- Running Economy: Injury Prevention Meets Performance
- Fatigue As A Biomechanical
- Footwear
- The Myth Of Perfect Running Form
- Decision Framework For Injured Runners
- Three Things To Do This Week
1. Overuse Injuries: How Running Injuries Really Develop
Most running related injuries are overuse injuries (Kakouris et al., 2021). These injuries aren’t a result of a traumatic injury, like an ankle sprain from a fall, but rather the result of repeated loading over time that leads to tissue maladaptation (Soligard et al, 2016). They build up gradually when your body is exposed to more running stress than it can recover from. This usually happens when load increases faster than recovery.
This might be from:
- running more mileage than usual
- adding extra sessions per week
- increasing pace, hills, or intensity
- returning too quickly after illness, time off, or injury
- or trying to maintain training when sleep, stress, or recovery are poor
Individually, none of these are “bad”. The problem comes when change stacks up faster than your muscles, tendons, or bones can adapt. Each run adds a little more strain, but there isn’t enough recovery time in between.
If you think you might be dealing with an overuse injury, book in with us now to get a clear diagnosis , understand what’s driving the problem, and put a plan in place that keeps you running — not resting indefinitely https://www.evolverehabtherapy.co.uk/contact/
.
2. The Single Biggest Risk Factor: A Previous Injury
Of all the risk factors investigated in the running injury literature, one stands out as the most consistently identified: a previous running-related injury, particularly one sustained in the last 12 months (van der Worp et al., 2015). Across systematic reviews, this finding appears more consistently than many other proposed risk factors – including age, sex, and training volume in isolation – which show far more conflicting results between studies.
A prospective cohort study of recreational runners with a history of running-related injury found that 55.1% sustained a new injury during follow-up – more than one in two (Fokkema et al., 2023). Over 20% of those new injuries occurred at the same anatomical location as the original injury, suggesting that the tissue itself retains vulnerability long after symptoms have resolved. Registration for a marathon event was also identified as a significant associated factor, reinforcing that previously injured runners taking on high training demands are at particular risk.
Why does a previous injury predict a future injury so strongly? One possible explanation is incomplete rehabilitation. When pain resolves, runners frequently return to full training, but tissue capacity has not been fully restored, carrying deficits in strength, endurance, or motor control. Returning to the same load that caused the original problem, without addressing the underlying capacity deficit, makes recurrence far more likely. Incomplete rehabilitation – resolving symptoms without restoring tissue capacity – almost guarantees a repeat problem.
? If you are returning from a running injury, book in with us now for a full assessment of your tissue capacity and a structured return-to-running plan. The question is not just “is the pain gone?” but “is the tissue ready?” These are very different questions, and answering the second requires proper assessment, not just time
https://www.evolverehabtherapy.co.uk/contact/
.
3. The Two Loads Every Runner Needs to Understand
in training and competition. It includes external load (what you do) and internal load (how your body responds).
External load usually involves calculating the training load, such as hours of training, distance, pace, frequency, whereas internal load is the physiological and psychological response to the external load, therefore includes measures such as heart rate or rate of perceived exertion.
External Load — What You Do
- Total distance (km per week)
- Running pace and intensity
- Elevation gain (hills and gradients)
- Training frequency (runs per week)
- Running surface (road, trail, track)
- Session duration and structure
Internal Load — How Your Body Responds
- Heart rate during and after sessions
- Rate of perceived exertion (RPE)
- Muscle soreness and fatigue levels
- Sleep quality and quantity
- Psychological stress and life load
- Recovery markers (HRV, resting HR)
Load management is a major risk factor for injury (Soligard et al., 2016) so it is important to monitor both types of load as you train. You could complete the same external load session in two consecutive weeks but respond with a different internal response. For example, a runner logging 60km per week in peak health, sleeping well and feeling fresh has a very different injury risk to a runner logging 60km per week while sleep-deprived, stressed at work and returning from a minor illness, even though the external load is identical.
These days wearable technology allows us to monitor our external and internal loads in real time, although there may be some inaccuracies measuring indications of internal loads so take the results with some caution.
Practical implication 1: Adjust your external training load in times of high life load (major work deadline, reduced recovery, emotional stress etc) as your body’s capacity to absorb high training load is reduced.
Practical implication 2: Share your monitoring with your coach if you have one. This way they can use your information to inform your training program to reduce risk of injury and increase effectiveness.
4. The Acute vs. Chronic Workload Ratio — Your Injury Risk in a Number
One of the most practically useful frameworks in load-management is the Acute vs Chronic Workload Ratio (ACWR) (Gabbett, 2016). This is the relationship between acute load (short term training) and chronic load (longer term average). It aims to show whether your recent training is a sensible step up from your established base, or whether it is a risky spike. Spikes in training load that are roughly 50% or more above your recent average are consistently associated with higher injury risk.
In simple terms, acute workload is the volume of what you have done in the last seven days. Chronic workload is your average weekly load over the previous four to six weeks. Divide acute by chronic and you get a ratio that suggests whether you are training within your recent capacity.
The specific numerical thresholds below should be treated as approximate guides, not hard clinical cutoffs.
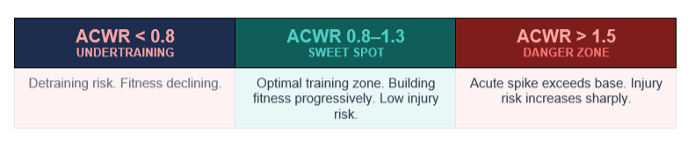
In practical terms: if your weekly mileage over the past four to six weeks averages 40 km (your chronic load) and you suddenly run 70 km this week (your acute load), your ACWR is 70 ÷ 40 = 1.75 — a spike most practitioners would treat as high risk.
5. Why the Same Training Error Causes Different Injuries
A common question in clinic is: “Why did I get a shin issue and not an Achilles issue, when the training mistake was the same?” The short answer is tissue-specific tolerance. Different tissues respond to different qualities of load and that is why the same error can produce different injuries in different runners.
- Shin splints
- Tibial stress fractures
- Metatarsal stress fractures
- Achilles tendinopathy
- Patellar tendinopathy
- Plantar fasciitis
- Myotendinous junction injuries (e.g. gastrocnemius)
- Hamstring tears
Case example – Tendon: A 35-year-old club runner with a consistent 50 km weekly base introduced two interval sessions per week ahead of a spring 10 km race, without reducing their existing volume elsewhere. After three weeks, they reported morning stiffness and a dull ache in the Achilles tendon – easing after 5–10 minutes of movement, then returning after longer or faster efforts.
This “warm-up” pattern is characteristic of early Achilles tendinopathy, where the tendon is reactive to increased load and symptoms are still potentially reversible with appropriate management.
High-speed running substantially increases the energy storage demands placed on the Achilles with each foot strike. Tendon adapts more slowly than muscle, and when high-intensity work is introduced too quickly, it may struggle to tolerate the increase. Prolonged complete rest is often counterproductive – the tendon requires ongoing, appropriately dosed loading to adapt.
The issue here was not the inclusion of interval training, but how it was introduced. Adding high-load sessions on top of an unchanged training volume created a sudden increase in tendon demand without allowing time for adaptation.
Key takeaway: Early tendon symptoms are an important signal, don’t ignore it – Modify the load – don’t remove it entirely.
Case example – Bone (Medial Tibial Stress Injury): A 38-year-old experienced ultra runner built their weekly volume to over 100 km – including regular back-to-back training days, in preparation for a 100-mile race in the Brecon Beacons. During the race, they developed a diffuse aching pain along the posteromedial border of the tibia, which gradually intensified and became more localised as the event progressed.
This pattern sits along the bone stress continuum, progressing from medial tibial stress syndrome toward stress fracture.Bone requires sufficient recovery time between loading cycles to remodel effectively. Back-to-back training days compress this window, limiting adaptation. During the race itself, prolonged cumulative loading combined with progressive fatigue reduced the capacity of surrounding musculature to absorb impact, increasing the mechanical demand placed directly on the tibia.
Terrain further contributed. Gravel and rocky surfaces can produce impact loading comparable to, and in some cases greater than, road running. Repeated descents increase tibial loading rates and bending forces, while uneven ground requires constant adjustments in foot placement. As fatigue develops, these adjustments become less controlled, increasing stress through the bone.
The progression from diffuse to localised pain during the event is clinically significant, suggesting that the bone’s tolerance threshold was being approached or exceeded.
Key takeaway: Bone injuries reflect cumulative load over time. When recovery is insufficient, especially with high volume, fatigue, and demanding terrain, stress can escalate from manageable irritation to structural injury.
6. Running Economy: Injury Prevention Meets Performance
Here is something that most injury-focused content misses: the same mechanical improvements that can lower injury risk also make you faster. Running economy (RE) is defined as the energy demand for a given velocity of submaximal running. It is strongly linked with performance and shaped by a mix of metabolic, biomechanical and neuromuscular factors (Barnes & Kilding, 2014).
Poor running economy costs you energy and increases injury risk. Consider overstriding — one of the most common mechanical inefficiencies seen in clinic. When a runner lands with their foot significantly ahead of their centre of mass, they generate a braking force with every step. A small cadence increase (often around 5–10%) can reduce braking and lower loads at the knee.
Strength training provides a clear example of this dual effect. Barnes and Kilding (2014) reviewed extensive evidence showing that resistance training improves running economy in trained distance runners by improving muscle-tendon stiffness. Simultaneously, better tendon stiffness means lower injury risk from repetitive elastic loading. The fastest runners are not just the fittest — they are also, biomechanically, the most resilient.
A more recent systematic review with meta-analysis by Llanos-Lagos et al. (2024) examined the effects of different strength training methods on running economy across middle- and long-distance runners. High load strength training (≥80% of one repetition maximum) and plyometric training both produced small but significant improvements in running economy, with moderate certainty of evidence for both. Submaximal load training and isometric training did not produce significant improvements in the same analysis. This matters practically: not all strength training is equivalent, and the intensity and method determine whether an adaptation occurs.
The case for strength training extends beyond economy. Leppänen et al. (2024) conducted a randomised controlled trial following 325 novice recreational runners over 24 weeks. A physiotherapist-guided hip and core exercise programme performed 2–4 times per week to muscular fatigue, produced a 39% lower injury prevalence and 52% lower prevalence of substantial overuse injuries compared to a control group performing static stretching. An ankle and foot exercise group in the same trial did not reduce injury rates — likely because the loading stimulus applied to those structures was insufficient to drive meaningful tissue capacity changes, consistent with the load-adaptation principles discussed earlier in this article.
Two important caveats apply to the Leppänen findings: the study was conducted in novice runners only, and the programme was supervised by physiotherapists. The protective effect was also specific to overuse injuries, not acute injuries. These factors limit how directly the results transfer to all runners — but the underlying principle is clear. Knowing which exercises to use, how to load them progressively, and how to integrate them alongside your running is where the expertise of a physiotherapist or strength and conditioning coach becomes essential.
Book in with us now if you want a personalised strength programme built around your running — one that targets the right structures, at the right load, progressed correctly alongside your training. https://www.evolverehabtherapy.co.uk/contact/
7. Fatigue as a Biomechanical Driver
One of the most consistent patterns observed in clinic is runners who describe symptoms appearing only at a specific point in their runs, typically the last third, or after a particular distance. “I’m fine for the first 10km but then my knee goes” is something I hear very regularly. Fatigue is almost always involved.
As a muscle fatigues, its ability to produce force diminishes. This has direct biomechanical consequences: the muscle can no longer stabilise the joints it crosses, absorb the shock it normally would, or maintain its movement patterns. The result can be a cascade of small compensations — the hip drops, the knee collapses inwards, the foot lands further ahead, trunk position changes. Researchers have found that running-related kinematic changes under fatigue, including increased hip adduction and contralateral pelvic drop, are directly associated with structures implicated in common injuries (Clansey et al., 2012).
Clinical significance: If your symptoms appear consistently after a certain distance, fatigue is likely a primary contributor. The question is not just “what is the structure?” but “why does this structure fail when it does?” This directs rehabilitation towards building muscular endurance not just strength, and towards improving running economy so muscles are under less demand at any given pace.
8. Footwear and Surface — What the Evidence Actually Says
Research by Nigg and colleagues (2015) has fundamentally reframed how we think about footwear. The traditional view was that running shoes correct biomechanical faults and reduce injury risk with cushioning and particular designs, however the evidence does not consistently support this.
Nigg’s research showed:
- that during a task, the skeleton of an individual athlete attempts to stay in the same movement path (known as the “preferred movement path”).
- that runners tend to stay in the same preferred movement path when running in different footwear conditions.
- that runners select a comfortable shoe depending on their own interpretations of what is comfortable, and that reflects natural alignment with their preferred movement path
- These are a better predictor of injury prevention than any specific biomechanical feature.
Shoes do not correct biomechanics. A stability shoe does not stop overpronation — it changes load distribution.
No shoe prevents all injuries.
Shoes influence how load is distributed. Comfort is a genuine signal — a shoe that feels right probably complements your natural gait.
Changing shoe type shifts load between structures and requires gradual transition.
9. The Myth of Perfect Running Form
There is no single ‘perfect’ running form, and deviating from an ideal does not automatically cause injury. Movement variability allows the body to distribute load across slightly different structures on each step, rather than concentrating it repeatedly on exactly the same tissues.
The goal is not perfect form but adaptable, resilient movement. A runner who moves with variability, maintains good tissue capacity through strength work, manages load intelligently, and recovers well will consistently outperform and outlast a runner who chases biomechanical ideals at the expense of the whole system.
10. A Simple Decision Framework for Injured Runners
Knowing what to change first is where many runners get stuck. Should you rest, run through it, strengthen, change your gait? It depends on the main driver.
| Primary finding | First priority | What this looks like |
|---|---|---|
| Sudden load spike (increased mileage, frequency, intensity, surface) | Load management | Reduce volume or frequency. Bring ACWR back into the 0.8–1.3 range before adding strength or gait work. |
| Identified strength deficit (weak glutes, calf, hip abductors) | Capacity building | Targeted strengthening 2–3x per week. Continue running at managed volume where pain allows. Expect 6–8 weeks for meaningful strength gains. |
| Persistent symptoms despite good load management and adequate strength | Gait retraining | 2D gait analysis to identify specific mechanical contributors. Cadence retraining, cueing, feedback. Strength training alone cannot change ingrained motor patterns. |
| High internal load despite manageable external load (poor sleep, high stress, illness) | Recovery & lifestyle | Address capacity-reducing factors first. Reducing training while sleep-deprived and stressed is smart periodisation, not failure. |
11. Three Things You Can Do This Week
Theory only matters if it changes behaviour. Here are three actions you can take this week, based on the principles above:
START HERE — THIS WEEK
1. Calculate your ACWR
Add up your running distance from the last 7 days and divide by your average weekly distance over the last 4–6 weeks.
If the result is above 1.3 — especially above 1.5 — hold or reduce volume before building again.
If returning from injury or time off, start back at no more than 60–70% of your previous weekly volume.
2. Add two strength sessions
- 3 sets of single-leg calf raises (slow, off a step)
- 3 sets of single-leg glute bridges
- 3 sets of lateral band walks
Under 20 minutes. Targets calf, glute medius, and hip abductor deficits common in injured runners.
Do this twice per week, not on back-to-back days.
3. Count your cadence on one run
Count how many times your right foot lands in 30 seconds and multiply by 4.
If it is below 160 steps per minute, try increasing it by ~5% using a metronome app.
Small cadence changes can reduce overstriding and may reduce knee load when introduced gradually.
Not sure where to start? Book in with us now. We will assess your load, movement, and strength, identify what is driving your risk, and build a plan that keeps you running — and gets you running better. https://www.evolverehabtherapy.co.uk/contact/
Key References:
Barnes, K., & Kilding, A. (2014). Strategies to improve running economy. Sports Medicine, 45(1). (PDF) Strategies to Improve Running Economy
Bertelsen, M.L., et al. (2017). A framework for the etiology of running-related injuries. Scandinavian Journal of Medicine & Science in Sports, 27(11), 1170-1180. A framework for the etiology of running‐related injuries – Bertelsen – 2017 – Scandinavian Journal of Medicine & Science in Sports – Wiley Online Library
Clansey, A.C., Hanlon, M., Wallace, E.S., Lake, M.J., (2012). Effects of fatigue on running mechanics associated with tibial stress fracture risk. Med Sci Sports Exerc 44(10):1917–1923. Effects of Fatigue on Running Mechanics Associated with Tibial Stress Fracture Risk – Ulster University
Kakouris, N., Yener, N., Fong D.T.P. (2021). A systematic review of running-related musculoskeletal injuries in runners. Journal of Sport and Health Science, 10(5), 513-522. A systematic review of running-related musculoskeletal injuries in runners – ScienceDirect
Gabbett., T.J. (2016). The training-injury prevention paradox: should athletes be training smarter and harder? British Journal of Sports Medicine, 50, 273-280. The training—injury prevention paradox: should athletes be training smarter and harder? | British Journal of Sports Medicine
Fokkema, T., Varkevisser, N., de Vos, R-J., Bierma-Zeinstra, S.M.A., & van Middelkoop, M. (2023). Factors Associated With Running-Related Injuries in Recreational Runners With a History of Running Injuries. Clinical Journal of Sport Medicine, 33(1), 61–66. https://doi.org/10.1097/JSM.0000000000001076
Lepänen, M., Viiala, J., Kaikkonen, P., Tokola, K., Vasankari, T., Nigg, B.M., Krosshaug, T., Werthner, P., Parkkari, J., & Pasanen, K. (2024). Hip and core exercise programme prevents running-related overuse injuries in adult novice recreational runners: a three-arm randomised controlled trial (Run RCT). British Journal of Sports Medicine, 58(13), 722–732. https://doi.org/10.1136/bjsports-2023-107926
Llanos-Lagos, C., Ramirez-Campillo, R., Moran, J., & Sáez de Villarreal, E. (2024). Effect of Strength Training Programs in Middle- and Long-Distance Runners’ Economy at Different Running Speeds: A Systematic Review with Meta-analysis. Sports Medicine, 54(4), 895–932. https://doi.org/10.1007/s40279-023-01978-y
Nigg, B.M., et al. (2015). Running shoes and running injuries: mythbusting and a proposal for two new paradigms: “preferred movement path” and “comfort filter”. British Journal of Sports Medicine, 49, 1290-1294. Running shoes and running injuries: mythbusting and a proposal for two new paradigms: ‘preferred movement path’ and ‘comfort filter’ | British Journal of Sports Medicine
Soligard, T., Schwellnus, M., Alonso, J., et al (2016).How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury British Journal of Sports Medicine, 50:1030-1041.How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury | British Journal of Sports Medicine
About the Author
Simone Passeri — HCPC Physiotherapist & MSc Sports Therapist
Simone is an HCPC-registered Physiotherapist and qualified Sports Therapist with an MSc in Physiotherapy (Oxford Brookes University) and an MSc in Sports Therapy (Buckinghamshire New University). He works with athletes and active adults recovering from musculoskeletal injury, post-surgical rehabilitation and performance challenges. He is a member of the Chartered Society of Physiotherapy (CSP) and Society of Sports Therapists (SST).


